What is The Balanced System®?
The Balanced System® is a whole system strategic approach to supporting children and people with a whole range of needs, that has primarily come out of work in the area of speech, language and communication but has evolved to be used to consider other therapy areas for children and young people, including occupational therapy, physiotherapy, CAMHS, holistic SEND support and most recently tests of concept with some adult populations.
This page outlines the core framework. For more detailed information, publications and downloads please follow this link.
The Balanced System® Scheme for Schools and Settings is a complimentary school or setting accreditation scheme that facilitates schools, settings or child minders to use the Balanced System framework to develop and evaluate their support for the children and young people they support.
Marie Gascoigne has been developing the Balanced System® framework for approaching 20 years. It is used by a whole range of stakeholders, including commissioners from all disciplines and providers, particularly of therapy services.

The graphic summarises the whole system framework starting at the bottom with the three building blocks.
- Jointly agreed outcomes commissioned for children and families. In the current legislative context that increasingly means jointly commissioned where possible, so asking various constituencies who have money, who have responsibility for making sure that services are available, to do that together and setting clear outcomes that they share for children, young people and their families.
- Whatever these outcomes are, to achieve them, we need an integrated workforce. There has been emerging recognition over the last decade that you can't, as a professional, achieve something on your own from just your professional perspective. It invariably involves working with colleagues and indeed with families and young people themselves.
- Crucially, parents and carers, families and children and young people, as core partners that underpin any whole systems approach.
Leadership forms a fulcrum right at the centre of the model. Over numerous reviews looking at collaboration around speech and language and other children's services, although hard to quantify and evidence in a formal way, it has been consistently reported that where there were strong local champions and leaders, services flourished and where that wasn't the case, the opposite, sadly, was also true. The Balanced System framework therefore recognises and emphasises its importance.
Sitting on top of everything is the service delivery framework itself. Training and development is a core plank that underpins all that goes above, then we have the universal, targeted and specialist levels of support which are delivered together by a wider workforce and a specialist workforce. All parts of the workforce have a contribution at all three levels, albeit their roles might be different and the specifics of what they do might be very different. All of these delivering outcomes across the Balanced System Five Strands.
The Five Strand Outcome Areas
The Five Strand Outcomes areas each with outcomes at a universal, targeted and specialist level, provide the High Level Outcomes Framework that a system working in this way should aim to be achieve.

Family support: supporting families, children, and young people themselves as they get older, with information, with skills and with advice to actually make decisions and build, resilience and be in charge of the situation in which they find themselves.
Enabling environments: where children and young people live, learn and have leisure, whether that be the home, a community environment, school learning environments etc. In an ideal world these need to be audited, adapted and enhanced to allow children and people with speech, language and communication needs (or other needs if you are looking at it through a different lens) to access and participate as much as possible.
Confident and competent workforce: to support children and young people. For that we need to acknowledge the fact that there are specialists in the workforce. We have to make sure that there are enough specialist competencies in a skill mix, but also that knowledge transfer and capacity building is happening so the wider workforce is continually being refreshed and renewed with skills that they need in order to support packages around children and young people.
Early identification and Effective Intervention. They are two, but only two, of the five strands. Intuitively and historically the focus has been on intervention in particular, and to a slightly lesser degree, identification. The core principle of the five strands model is that identification and intervention are only as impactful as they can be within that whole system, and acknowledging that there has to be a context of family, environment and workforce in which they happen.
Our identification needs to be as efficient and as accessible as possible. That involves making sure that people in the wider workforce have support to know what to look for, to bring the right children through, but also that we don't put unnecessary barriers in the way of access to services. If we can quickly see something that will help, we should be able to move a child or young person through to that offer even if we think there are elements that need more exploration.
Our interventions need to be appropriate and timely. Whether direct, indirect, individual or group, there needs to be a core functional purpose. We know from research like the Better Communication Research Programme that families value things that they can see are making a difference in their child's life in terms of their wellbeing, their confidence and their participation whilst accepting the importance of working on other areas. Those outcomes are what matter to families.

Is it making a difference?
To think about how we might measure what we do, we've used the well documented model from American economist Friedman. We’ve taken the quantity, quality, effort and effect grid and given a layer of language that is more appropriate to our needs into describing what the different quadrants are about.
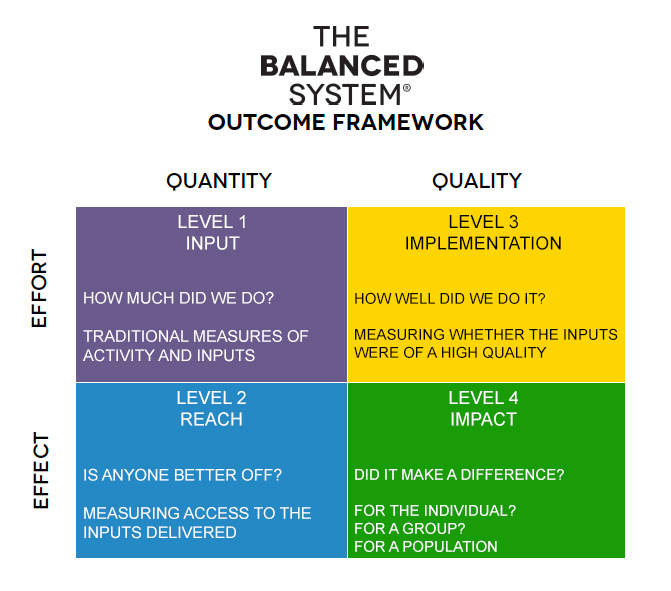
The first quadrant is called level one and is an input measure; it's about measuring how much we did through traditional measures of input such as face to face contacts, etc. These measures have a value. They tell commissioners and contract managers that something happened, but they don't tell us whether it made any difference. That’s a key leap to think about and something we work on with commissioners using this framework.
Staying on the quantity side of the grid, the quadrant below is level two: reach. This stays with the notion of counting but means: did we set goals as to how many of these things we wanted to do, for how many people and who these people are? How well are we doing in getting to that reach: was it 100% of what we set out to do or was it 80% or 70%.? This gives us more meaningful information, but is still very much about the activity and input rather than the impact.
We then move over to the quality side, and we have level three: implementation, which is around the quality of what we've done. For instance, was it good training? Was it a good, well-planned intervention?
Sadly, it can be excellent but still not making a difference to the child or young person, for a whole host of reasons. This is not about being critical, it's saying that we need to recognise that possibility and try and move to include some measures that are about impact. So did we make a difference? Can we show that we made a difference? Can we Prove It? Whether that difference is for an individual, for a group such as a specific intervention group or a class or a school, or even going up to a population at a much broader level.
The length of time that we will need to have those measures in place will vary depending on what it is we're trying to measure and at what level. Population measures, naturally, will require trend data that might take a number of years to provide evidence. Building a measurement framework is not about the specific tools; you could use a whole range of tools to get those measures. The key is to have a system that allows us to consider all aspects: have we got a measure for impact or are we even setting out to measure impact?
For more information on impact measurement see the Prove It! platform
All of this comes together in Integrated Solution Tool.
The Integrated Solution Tool and Core Delivery Principles
The Integrated Solution Tool considers what is needed in a whole system to deliver to the shared high level outcomes.
For each of those outcome areas, we then need to work through:
- what the overall outcome looks like - how will we know it has been achieved?
- what the outputs might look like that one would need to produce in order to achieve those outcomes, the likely tangible things that would need to be exist in the system
- what the processes be required to make it happen. This is personalised to the particular context in a particular area or service, or whoever is using this from whatever angle, to get it right for the circumstances, area of focus and local context
- what impact measures will need to be in place to evidence the system is delivering the outcomes?
We then need to try and specify who has to do what in order to achieve this outcome. A core principle which is fundamental to the Balanced System® framework is that no outcome can be achieved just by one element of the system. There isn't an outcome that just speech and language therapists can solve, or just specialist teachers or EPs or health visitors or SENCOs. There isn't an outcome that can just be solved by good teaching or by parents doing their best and working as hard as they possibly can. It needs a collaboration, and that collaboration will have a different mix and a different balance for each outcome at different levels but there is always going to be a mix required.
In the Integrated Solution Tool, for every one of those outcomes are worked through examples of what you might see, how you might do it, how you might measure it, what you'll need from your speech and language therapist, your SENCO or your health visitor, your class teacher or your nursery nurse and what parents will need to do. The context section is about other things like space and capacity and perhaps support from senior leadership etc.
Core Delivery Principles
The core delivery principles for change are based on the five key elements that typically need to develop in order to move to a system offer in a local area that meets the high level outcomes across the Balanced System® Five Strands and Three Levels.
Establishing these five delivery principles in a system offer facilitates access to therapy at the appropriate level, including specialist therapy, by ensuring that the system is being as accessible, integrated and impactful as possible.
Delivery Principle 1: Focus on functional outcomes and measures of impact
The whole delivery model is underpinned by a focus on delivering functional outcomes – the ‘so what?’ and measuring impact not inputs rising to the ‘Prove It!’ challenge
- Child and young person outcomes
- Family outcomes
- School, setting, class or group outcomes
- Area cohort outcomes
- Population outcomes
Delivery Principle 2: Access
Simple and easy access to the right information, assessment and support for children, young people and their families
- Early identification - meaning not only early in life but early in the emergence of need at any age
- Easy access - simplest route to support at the lowest level even if further progression through the system required
- Appropriate assessment - enquiry based process, with the option to signpost to appropriate support that may be part of the whole even if further assessment is indicated
Delivery Principle 3: Placed based support
Support is delivered in the most functionally appropriate and relevant place for the child or young person, their development, learning and leisure.
- Resources are allocated based on need – differential in either or both the nature of the offer or the volume of the offer based on evidence of need
- Link therapist - meaning a school or setting based key therapist whose time is consolidated into their schools and settings and who work regularly as part of the school or setting team
- Intervention focused on functional outcomes - the therapeutic offer must be focused on functional, ideally child and family or young person led, outcomes
Delivery Principle 4: Build the targeted offer as part of the continuum of support
Development of strong universal and targeted provision is key to facilitating access to specialist support as and when needed for a finite time
- Targeted offer – building a robust targeted offer across all five strands is key activity for all: SLT or other therapy team alongside the wider workforce
Delivery Principle 5: Information
High quality, accessible and consistent information and advice are available in a range of media and culturally appropriate forms to enable parents and carers and professionals to be well informed. These typically have been quality assured
Examples of delivering the Balanced System® Principles in Early Years
- Link therapist for clusters of early years settings linked with community bases such as Children’s Centres or Family Hubs
- Close working with Health Visiting colleagues re early identification
- Easy access for families to advice and support and regular drop-in sessions for initial advice, signposting, initial informal assessment and where appropriate direction to more detailed assessment. Drop-ins can be used to facilitate direct access to universal and targeted support.
- Development of targeted offer in locality systems for early years to ensure there appropriate opportunities for families to access
- The support we offer needs to be focused on functional outcomes that are the priority for the individual and their family at that time
Examples of delivering the Balanced System® Principles in Schools
- Link therapist for every school who really gets to know the school and is the lead point of contact for the school around any of the SCLN needs of children in the school
- All children and young people of school age assessed in their learning context – the ‘so what?’ is to be able to use SLT expertise to unpick what they need to access the
curriculum, be socially integrated with peers and thereby improve mental health and well-being - The support we offer needs to be focused on functional outcomes that are the priority for the individual and their family at that time – these may change frequently or stay the same for some time and that’s ok!
Examples of delivering the Balanced System® Principles from a service perspective
- The offer to the school should be across all strands and levels not only on a child by child basis – that way the collaboration around one child builds learning in the school for many children to come
- Service needs to allocate resource to schools based on need - resources are finite - school may choose to enhance the offer
Population, intervention and workforce
How does this fit together in terms of who does what and for whom?
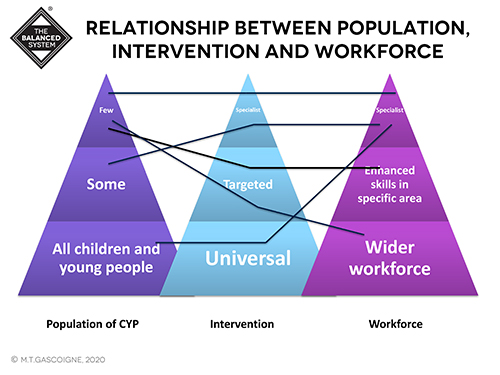
The first pyramid diagram shows a population of children and young people. Based on research data, we can say what we expect to find in any population of children and young people in terms of different kinds of speech and language needs or other needs if looking from the perspective of other therapies or wider SEND.
There will be a relatively small number (relative to the whole population) which will have complex and specific needs.
We can expect to find a larger group with more varied needs that are still significant. Inside that larger group would be children and young people who have specific needs in an area such as speech, language and communication and others whose primary needs may be in other areas with speech, language and communication as part of their overall profile.
There will be a much larger group which is more varied in terms of needs. Some will go on to be identified as having more significant needs but we know that there are children who, through disadvantage or lack of early experience or various factors that are perhaps not as well understood as they will be in the future, will be more likely to have speech and language needs, particularly in the early years. So the bottom of the pyramid is a larger group of children and young people, which will vary from situation to situation, many of whom can be expected to respond well to support and then move down the pyramid to not having any needs, as opposed to moving up if those needs are not addressed early.
The middle diagram is the pyramid of universal offer and targeted and specialist interventions. In the whole systems approach, some of the things that we do for children and young people will be to enhance and manipulate the universal and the general environment that all young people experience, some will be about targeted interventions and some will be specialist. There is debate around exactly where the lines are drawn between targeted and specialist but it is recognised that there is a continuum of intervention support.
The third pyramid shows the workforce ranging from the wider workforce, which is absolutely everybody, through to those that have developed enhanced skills in a particular area. In the case of speech and language needs that might be a teaching assistant that has completed a Level Three qualification in speech and language and developed lots of enhanced skills through to the specialist workforce of speech and language therapists, specialist teachers, EPs etc.
We have a range of ways of travelling across these three pyramids. There might be, for example, a child with quite complex needs who sits in that 'few', but whose needs are appropriately met by targeted interventions at the moment, delivered by either somebody with enhanced skills or potentially even through the wider workforce. At the same time, we might have a young person who has a less complex profile and sits further down the population pyramid, but for whom a specialist intervention delivered right now might be really effective and make all the difference, and might even be all that they're ever going to need.
Equally, when we're looking at the universal offer and enhancing the universal provision that's out there for all children and young people, we might need specialists to be the people doing that, because they may have better training and knowledge to impart their specialist knowledge in that wider context. We want to avoid the assumption that we travel horizontally across these three pyramids. We do sometimes, but it shouldn't be the default.
What does a child or young person’s journey look like?
If we think about what a journey might look like and what the provision itself might feel, if we consider all the processes and outputs that sit in the Integrated Solution Tool we're talking about many, many units of activity that you could define as separate units. For any child at any one time accessing any element of the service, they're likely to be accessing perhaps six or seven of those simultaneously and they might be coming from all different levels.
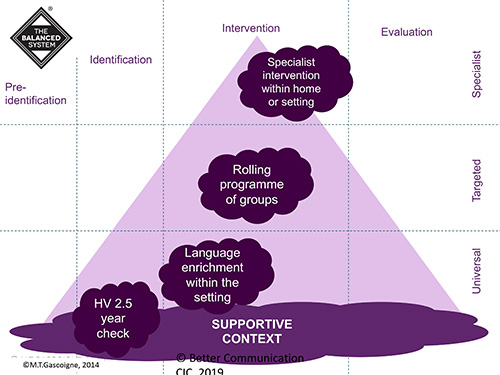
To illustrate, this diagram shows the three levels on a vertical axis and the notion of time from left to right: things to do with pre-identification which is information and awareness raising generally, things to do with identifying which is specific to particular individuals or groups, things around intervention and things around evaluation.
The two and a half year Health Visitor check is a universal identification activity, as it happens for everybody and it's definitely about identification. However, if we're thinking about that whole systems model from a commissioning perspective, if the outcome is around identification and a core component is that the Health Visitor does their two and a half year check, the Health Visitor has to be supported at some level by training, by confidence in their own competencies to actually do the identification. That will undoubtedly involve professional collaboration with speech and language colleagues, or even training delivered by speech and language therapy colleagues, which will have to be funded and commissioned in order for the whole thing to work. They need to be therefore identified as clear components of what's needed in the bigger whole.
Let’s think about a language rich environment within a school or a nursery setting. A Health Visitor might see a child at two and a half and think “I don't think a speech and language referral is needed here, but they definitely would benefit from a little bit of experience and enrichment. So I'm going to direct the family to a setting that has a particularly good language rich environment.” That language rich environment won't come about by accident; it would have needed staff training, consideration of the environment and whether the environment is suited to enabling and communication friendly and so forth. That might involve training from speech and language therapy service or from other colleagues, bringing in materials that have been sourced or might be available nationally, but all of those things have to be there in order for it to happen.
Thinking more specifically, we might have a targeted intervention like a rolling programme of groups. For example, a speech language service can predict that there are always going to be children that require attention and listening support, vocabulary development and certain speech sound system issues that are common. So rather than organising your service around who comes to the door you might decide to set these group up and have these running. In an ideal situation you would be doing that collaboratively with schools and settings where those young people might be.
Then, of course, there are situations where a specialist intervention is required. Here the example is within a school setting where you might have a specialist intervention going on and indeed, the child that's receiving that specialist intervention might also be accessing a group in the rolling programme. They may also be benefiting from a language rich environment and may have been identified at two and half years old by their health visitor.
All of this is to illustrate the fact that we need to think more flexibly. We don't want the pathways that we have to become silos. For example, if a child in the identification part of this model were felt to need a specialist multidisciplinary assessment that required a longer wait but it was obvious that they would also benefit from accessing something at a targeted level immediately, that should be possible. They shouldn't be sort of hived off into a pathway that becomes confining, as opposed to doing something in the meantime while moving forward towards that more complex identification. It's thinking more fluidly about things.
See also the Balanced System Pathway Tool